
Author: Kevin Gurr
published with permission
Fact Closed-circuit rebreathers (CCRs) are popular in advanced recreational diving owing to advantages such as minimisation of gas consumption and the optimising (reduction) of decompression. Rebreathers recycle expired gas around a closed loop circuit using one-way valves. Expired carbon dioxide (CO2) is removed as it passes through a ‘scrubber’ canister containing CO2 absorbent. The most commonly used absorbent is soda lime (a mixture of sodium hydroxide and calcium hydroxide).
Rebreathers are more complex than open-circuit scuba equipment and can be prone to operator errors. Some of these relate to the CO2 scrubber and its use. The absorbent material has a finite capacity and must be changed regularly. Errors include failing to replace the absorbent material when required, incorrect packing of the absorbent canister, incorrect installation of the canister in the rebreather and, rarely, forgetting to install it (or the material) entirely. Such errors may allow expired CO2 to enter the inhaled gas which may in turn cause symptomatic CO2 toxicity (hypercapnia). Hypercapnia is also known to speed the onset of oxygen toxicity and the narcotic effect of nitrogen breathed at higher partial pressures.
How do we deal with increases in CO2? A simple but crucial physiological fact is that CO2 is eliminated by breathing. The brain (which detects CO2 levels in the arterial blood) aims to match breathing with CO2 production to keep levels in the body stable. Thus, if CO2 production rises, the brain should drive more breathing to eliminate it, and vice versa. However, under conditions of increased work of breathing (especially combined with exercise) the brain may subconsciously choose not to perform the breathing work required to keep CO2 normal, and CO2 levels may rise. Some people (often referred to as “CO2 retainers”) are more prone to this than others. Work of breathing is affected by depth (gas density) and the breathing resistance within the breathing loop. To illustrate the effects of this, in a study [1]test subjects were exposed to varying levels of inspired CO2, exercise and breathing resistance. Three results were summarized as;
- Elevated CO2 with breathing resistance added, produced an increased ventilation that moderated (but did not stop) CO2 increase
- No CO2 but elevated resistance added produced no rise in ventilation rate and CO2 retention occurred as in a working (functioning scrubber) rebreather with excessive breathing resistance
- Moderate depths (18 meters) was been shown to reduce the effectiveness of ventilation in removing CO2 due to gas density, lung stiffness etc. and therefore the ability to control CO2 through increased ventilation is reduced with depth
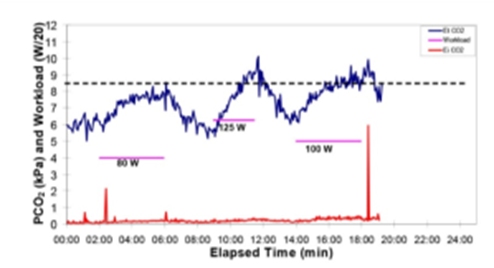
In summary, in considering the effectiveness of CO2 removal, a secondary factor related to the breathing resistance (Work of Breathing/WOB) of the rebreather must be considered and this increases with depth. The effects of exercise on CO2 retention were further expanded on in a study (See figure 1) referenced in the graph below. The red line records the CO2 passing through a scrubber canister (the spikes are analyzer calibration runs) and clearly show that the scrubber is functioning correctly (almost no CO2 breakthrough). The blue line references CO2 measured at the end of each breath (end tidal CO2); this reflects CO2 levels in the body. This was recorded at three work rates (80watts, 125watts and 100watts). The dotted black line is the maximum allowed limit of end tidal CO2 (a PCO2 of 8.5 kPa) and the graph clearly shows that while the scrubber is functioning perfectly, the end tidal (retained) CO2 rises above acceptable limits as workload increases. The crucial thing to realize about this is that exercising at surface pressure does not cause an increase in body CO2. The difference here is that the diver is breathing a denser gas (nitrox at 40m) through a rebreather which increases the work of breathing. This is an illustration of the point made above that the brain has made a subconscious choice not to perform the extra work required to breath has hard as necessary to keep the CO2 normal.
[1] Courtesy Anthony Garvin
Work of Breathing Work of breathing (WOB) put simply is the effort required to move gas around the breathing loop. It is a combination of the resistive (restrictive) elements of the loop (small hoses etc.) and the pressure difference (distance) between the counterlungs and the lung centroid [1]. This distance adds to the resistive element and changes as the diver rotates in the water. WOB also increases with depth and gas density because more effort is required to move gas through the airways and equipment. As previously discussed, elevated WOB can lead to CO2 retention Linked to this, gas density trials have been conducted where groups of divers were exposed to increased gas density while exercising underwater in rebreather tests. If the diver’s end tidal CO2 level rose to 8.5 kPa or higher, that was considered a failure due to CO2.
[2] A notional pressure point at the centre of the lungs against which pressure readings are referenced
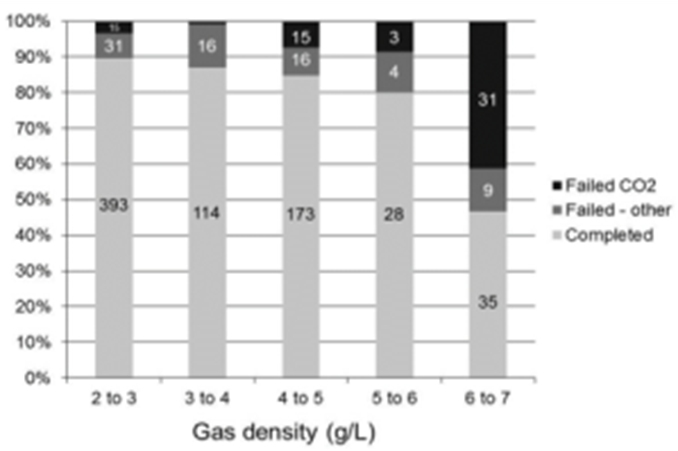
[3] Courtesy Gavin Anthony The shown graphfigure 2 details a series of tests at increasing gas density (measured in grams/litre (g/l)). For reference, air breathed at surface pressure is about 1.23 g/l. Looking at the first column where the gas density was 2 to 3 g/l, 439 tests were completed. 393 completed successfully, 31 failed for reasons other than CO2 issues and 15 (3.4%) failed because of high CO2. Conversely the last column where the gas density was 6 to 7 g/l, only 35 completed successfully and 31 (41.3%) failed due to CO2. Therefore, the elevated gas density which in turn created an elevated work of breathing generated high failure rates. The study suggests that ideally gas density should be below 5.2 g/l or air at 31m and definitely not exceed 6.3 g/l or air at 39m. Fiction The following items can be considered as common misinformation and should be treated accordingly. In short all of the below are NOT true.
- All CO2 absorbent is of similar design and generates similar performance. Therefore, I can put any absorbent in my rebreather and it will perform within the manufactures published limitations. Author’s note: There is a large selection of CO2 absorbents used across the medical, diving and other industries. Each has unique properties ranging from shape and construction through to chemical makeup and water content. Only Diving Grade absorbent should be used for diving.
- The published CO2 endurance times for my rebreather can be conducted at any depth, in any water temperature and at any work rate. Therefore, these three variables do not have any effect on the ability of the scrubber to remove CO2. Author’s note: Scrubber endurance can be massively affected by these variables. In addition, each rebreathers specific design can affect the endurance so a duration obtained with an absorbent type in one rebreather will not be the same in another rebreather.
- One type of scrubber design (be it radial, axial, cross flow etc.) will always perform better than another. Author’s note: Historically it was thought that radial designs always gave better performance, but this is not universally true and in reality, axial designs are often better performers.
- Post dive, rebreather absorbent can be removed, dried and refitted to improve performance. Author’s note: This is VERY dangerous.
- I can store a part used scrubber indefinitely and use again and obtain the same performance. Author’s note: The variabilities of container integrity and water content loss (evaporation) make this a dangerous assumption. Formal testing of partly used absorbent has shown almost no degradation in unprotected overnight storage, and very little degradation in air-tight storage for a month, but prolonged unprotected storage results in substantial degradation.4 Prolonged air-tight storage (> 1 month) has not been properly tested and should not be relied on.
- Advanced CO2 absorbents such as lithium hydroxide can be safely used in a recreational rebreather. Author’s note: Lithium hydroxide (while very efficient as an absorbent) is an extremely volatile chemical composition and reacts aggressively with water. It should not be used in rebreathers.
- Out of date absorbent, as long as it is in a sealed container, can be used. Author’s note: Again, this procedure cannot be relied on. Out of date medicines would not be used, so the same applies to absorbent material.
- In a breathing loop the CO2 scrubber is the most important element for managing CO2 around the loop. Author’s note: Obviously the scrubber is vital for removing CO2 but even a partly used or poorly packed scrubber is not as dangerous as a failed mouthpiece mushroom valve. The first test of any rebreather setup should be for mushroom valve integrity.
Voodoo Comparing endurance Divers obviously need to know how long their rebreather will continue to remove CO2 from the loop in use and manufacturers would ideally want to quote a duration as guidance. This is difficult to quantify because a rebreather scrubbers’ ability to remove CO2 is a function of several variables;
- Work rate (metabolism and therefore CO2 generation)
- Ventilation rate (primarily as a function of work rate)
- Water temperature
- Absorbent type
- Rebreather design (primarily as a function of heat loss)
- Depth (primarily as a function of gas density)
This often creates a dilemma, especially for manufacturers. The ideal solution would for all manufacturers to quote an endurance based on a worst case scenario. This would then create a ‘level playing field’ from a user information/safety standpoint. This is exactly what the CE test standard for rebreathers (EN14143) tries to do, in that it uses the following parameters as a test requirement;
- 6l/min CO2
- 40l/min ventilation
- Water temperature 40C
- Depth 40m (an additional test at 100m is used for heliox/trimix rebreathers)
- Diluent air
The current reality is that test results obtained using these parameters do not make some rebreathers ‘look good’ from a performance perspective in that they do not live up to their manufacturers initial design expectations, this creates a marketing issue. Often the end result is that within operating instructions, while testing to EN14143 will be referenced in a manual, there will be a caveat that references a change in the parameters such that the endurance figure is increased. While the CE parameters are arguably extreme in relation to sport diving they do provide a good safety net and especially for Technical diving profiles and/or when high work rates are experienced towards the end of a scrubbers life. The end result is users must beware when comparing rebreather performance and should check with the manufacturer if there appear to be any ambiguities at all in the quoting of endurance figures.
The 5 minute pre-breathe Historically, a scrubber integrity test conducted by divers is to breathe an assembled unit for 5 minutes in order to generate symptoms of hypercapnia experienced as a result of a failing scrubber or sealing system that in turn may create a ‘bypass of CO2. This process has several issues such as ‘how large’ is any bypass and can we physiologically detect that level? In a trial completed in New Zealand, the following observations were noted. The five-minute pre-breathe is an insensitive test for CO2 scrubber function in a diving rebreather, even when the scrubber canister is absent. A pre-breathe is nevertheless recommended for purposes such as checking the function of the oxygen addition system before entering the water, but a duration less than five minutes should be adequate for that purpose. Arguably the most important secondary finding of our study is that partial scrubber failure in a rebreather is a particularly insidious fault if divers rely on a pre-breathe to detect it. By modestly increasing ventilation, subjects typically maintain normocapnia during a surface pre-breathe in this condition, resulting in a false negative that is dangerous because normocapnia is much less likely to be maintained during the dive itself. The observations from this trial point to the fact that the only reliable test of a scrubber systems integrity should utilize a gaseous CO2 sensor.
All absorbents are the same As previously mentioned, there are several manufacturers and types of commercially available absorbent. A common misconception is that ‘absorbent is absorbent’ and one will last just as long as the other. Again, in a New Zealand trial, two common diving absorbents were tested.
Author’s note. These tests were completed at surface pressure and testing at depth will change the results although the relationships will remain broadly the same. Sofnoline 797[4] (maximum granule size 2.5mm) and Spherasorb[5] (maximum granule size (5mm) were tested with the following results.
[4] Trademark Molecular Products Ltd
[5] Trademark Intersurgical Ltd
The mean operating duration to CO2 breakthrough was 138 +/-4 (SD) minutes for 2.38 kg of Spherasorb and 202 +/- 4 minutes for 2.64kg Sofnolime (these different weights of the respective materials occupied the same scrubber volume and were different because Spherasorb has a larger granule). The difference between the peak respiratory pressures was 10% less during use of Spherasorb, suggesting lower work of breathing. Under conditions simulating work at 6MET during use of an XX rebreather a canister packed with Spherasorb reached CO2 breakthrough 32% earlier with 10% less mass than Sofnolime packed to similar volume. Divers cannot alternate between these two preparations and expect the same endurance.
The scrubber ‘curve’
When tested at a steady depth, temperature and CO2 generation rate, the CO2 ‘curve’ is mostly a flat line (0mb CO2) for at least 2/3rd of the endurance time. In the last 1/3rd it starts to rise until it passes the 5mb and then 10mb safety alarm limits[6]. The ‘lift’ towards 5mb often only occurring in the last 10-15% of the endurance time and the rise to 10mb in the last 10-20 minutes or so. At first glance it would appear that we can safely exercise right up to nearly the end of the scrubber life without a bypass taking place, even at the extreme CE test rate and or having ill effects due to hypercapnia. The reality is not so simple and can depend on several elements such as rebreather design, increased ventilation rate in addition the increased ventilation can produced an increase in work of breathing and the associated CO2 retention, especially at depth. Unmanned trials do however indicate that in the first 2/3rd of the scrubber life, even with increased ventilation/work-rate that the scrubber can ‘cope’. However, it is clear that this is not always the case in the final 1/3rd.
CO2/endurance sensing Gaseous CO2 sensor are not new and have been used in surface applications for years and are a way of instantly measuring CO2 in a breathing loop. More recently a form of CO2 sensor has been used for diving with rebreathers. It is known as a non-dispersive infra-red (NDIR) sensor. Put simply, using infra-red light it measures the spectral response of CO2 when the light is passed over it. Unfortunately, the spectral response of water is similar to CO2 and can also be detected. This can create a ‘false positive’ (high reading) and a shorter dive endurance, which in itself can be seen as a ‘fail safe’ scenario. Some manufactures have successfully integrated NDIR sensor in rebreathers with additional moisture filtration, sometimes at the expense of sensor response time and long duration use (due to filter degradation) is still potentially an issue. Gas density can also affect these sensors but can in most cases be compensated for.

Another, less common sensor used uses a chemical gel patch which changes colour as more or less CO2 passes over it. This change is then measured and directly correlated to a CO2 level. These are less prone to moisture interference and are gas density independent. Gaseous sensors aside, a scrubber’s endurance prediction is the next challenge. Current systems rely on the fact that as absorbent is used within a scrubber housing, a thermal ‘front’ slowly moves through the scrubber tracking the active section of the absorbent. As that section is used, the front moves on. This thermal front movement can be detected using a series of temperature sensors (a thermal array) arranged linearly within scrubber. As each sensor peaks, then a percentage remaining can be estimated and compared to a tested endurance to predict time remaining.
[6] Reference CE EN14143

While thermal array monitors are a good steady state system, accuracy is challenged in shallow and warm water and it cannot predict bypass as a result of high workload. In short, all types of sensor have one issue or another that can also relate to how it is deployed within the rebreather. The only way to verify suitability is to review test results. In summary, gaseous CO2 sensors help with;
- Bad CO2 seal
- Bad absorbent
- Absorbent abuse (used too long, repacked)
- Breakthrough due to high work
Gaseous CO2 sensors do not help with;
- Detecting CO2 retention
- Duration monitoring
Thermal arrays help with;
- Endurance prediction
Thermal arrays do not help with;
- CO2 bypass as a result of high workload/seal failure
Choosing an absorbent The correct choice of a CO2 absorbent product may not be as simple as it first seems. For a lot of divers, cost is an issue for others, especially deep divers it might be endurance or work of breathing. The key point here is you need to decide what your objectives are and above all you should prioritise safety as the driver. As an example, if you are only conducting short, shallow dives then a product that is more cost effective at the expense of endurance may be applicable. If all your diving is in warm water, then again a less efficient product may be suitable. Conversely, if you diving is deep, long and cold then ideally would want the best performing product possible from an endurance perspective but again that should be balanced against any work of breathing issues of a potentially more densely packed (smaller granules) absorbent if that is the choice, much of the latter being mitigated by using the correct diluent at depth.

The bottom line with absorbent use is, you have choices, make them wisely. Consideration on long dives should also be given to the product’s ‘friability’, its tendency to break into smaller particles, bypass any scrubber filtration and mix with condensed water to generate a caustic cocktail. Friability is tested for by most manufacturers and can normally be simply evaluated by comparing how mush dust there is at the bottom of a used barrel of product.
Safety Top 10.
- Find out and understand the CO2 endurance limits of your chosen rebreather design
- Hypercapnia is insidious and potentially lethal – do not assume you can detect or ‘handle’ it.
- Use absorbent that has been qualified for your rebreather and is in date. Be fully conversant with the manufacturers test data. You have a right to ask, use it.
- Do not assume all absorbents give the same duration
- Understand the scrubber curve, avoid high work rates towards the end.
- Use the right gas at the right depth to minimize WOB and CO2 retention. Gas density should not exceed 6.2 g/L
- CO2 sensing is a major safety feature with extended use and changing workload. If at all possible, use a CO2 sensor
- While data suggests it is acceptable to store part used absorbent without protection overnight and in a sealed container for up to one month without significant degradation of the absorbents performance. This must be balanced against the guaranteed integrity of the storage system and the real cost/benefit of just replacing the absorbent. Overnight storage in a sealed rebreather is documented as being a practical option.
- Do not rely on the 5-minute pre-breathe as a CO2 system test, but do:
- Check mouthpiece mushroom valves on every dive
- Check CO2 seals
- Properly pack the scrubber
- Do not dive with a leaking rebreather, this will;
- Increase WOB
- Decrease absorbent efficiency
- May generate a caustic solution that could be swallowed
Summary
The current ‘state of the nation’ is that there are several types of absorbents available for use, only a small number of these absorbents have been tested and qualified in the now available larger range of recreational diving rebreathers. As a result, there is some confusion with regard to the safe limits of use. In addition, the complete picture of issues related to CO2 is a complex event and while elements of it are covered in isolation in most training documentation, the more ‘joined up picture’ is seldom discussed in detail. As a user group and as technology evolves, it is vital that we become as educated as possible with regard to the training and management of CO2. Whether choosing a new rebreather, a training program, a specific instructor or an absorbent supplier, it is important that we confirm the detail and validity of the information we receive.
Bibliography
- Shykoff SE, Warkander DE. Exercise carbon dioxide (CO2) retention with inhaled CO2 and breathing resistance. Undersea Hyperb Med 2012;39(4):815-28. PMID: 22908838.
- Anthony TG. Diving re-breathing apparatus testing and Standards: UK/EU perspective. In: Vann RD, Mitchell SJ, Denoble PJ, Anthony TG, eds. Technical Diving Conference Proceedings. Durham, NC: Divers Alert Network; 2009. p. 218-36. Available from: https://www.diversalertnetwork.org/files/Tech_Proceedings_Feb2010.pdf
- Anthony TG, Mitchell SJ. Respiratory physiology of rebreather diving. In: Pollock NW, Sellers SH, Godfrey JM, eds. Rebreathers and Scientific Diving. Proceedings of NPS/NOAA/DAN/AAUS June 16-19, 2015 Workshop. Wrigley Marine Science Center, Catalina Island, CA; 2016. p. 66-79. Available from: https://www.omao.noaa.gov/sites/default/files/documents/Rebreathers%20and%20Scientific%20Diving%20Proceedings%202016.pdf
- Pollock NW, Gant N, Harvey D, Mesley P, Hart J, Mitchell SJ. Storage of partly used closed-circuit rebreather carbon dioxide absorbent canisters. Diving Hyperbaric Med. 2018;48:96-101. doi: 10.28920/dhm48.2.96-101. PMID: 29888381. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6156827/
- Deng C, Pollock NW, Gant N, Hannam JA, Dooley A, Mesley P, Mitchell SJ. The five-minute prebreathe in evaluating carbon dioxide absorption in a closed-circuit rebreather: a randomised single-blind study. Diving Hyperbaric Med. 2015;45:16-24. PMID: 25964034. Available from: https://www.dhmjournal.com/images/Journals/45/DHM_Vol45_No1.pdf
- Harvey D, Pollock NW, Gant N, Hart J, Mesley P, Mitchell SJ. Comparison of duration of two CO2 absorbents in a diving closed-circuit rebreather system. Diving Hyperbaric Med 2016;46:92-7. PMID: 27334997. Available from: https://www.dhmjournal.com/images/Journals/46/DHM_Vol46_No2.pdf

Therebreathersite was founded by Jan Willem Bech in 1999. After a diving career of many years, he decided to start technical diving in 1999. He immediately noticed that at that time there was almost no website that contained the history of closed breathing systems. The start for the website led to a huge collection that offered about 1,300 pages of information until 2019. In 2019, a fresh start was made with the website now freely available online for everyone. Therebreathersite is a source of information for divers, researchers, technicians and students. I hope you enjoy browsing the content!