
Gibbs 2 hours apparatus Bureau of Mines USA
Text Jan WIllem Bech
rewrite june 2022

Introduction
The Gibbs 2-hour apparatus was designed by W. E. Gibbs, a mechanical engineer connected with Columbia University, while employed by the Bureau of Mines as consultant to develop an oxygen breathing apparatus that would embody ideas suggested by the experience of Bureau engineers and others and thus be safer and more efficient than the types in use. After experimental and development work had progressed to the point where a few apparatus had been built by hand, worn, and tested, permission to construct the apparatus was issued to an American firm. Some changes were made to adapt the apparatus to commercial manufacture; the manufacturer then submitted it to the Bureau for testing and approval, as provided for in Schedule 13 The Gibbs apparatus was formally approved February 15, 1920, for safety, reliability, and efficiency, and approval 1300 was issued to the Mine Safety Appliances Co., Pittsburgh, Pa., to cover it. After approval numerous changes were made by the Bureau and the manufacturer to improve various features.

Parts of the system
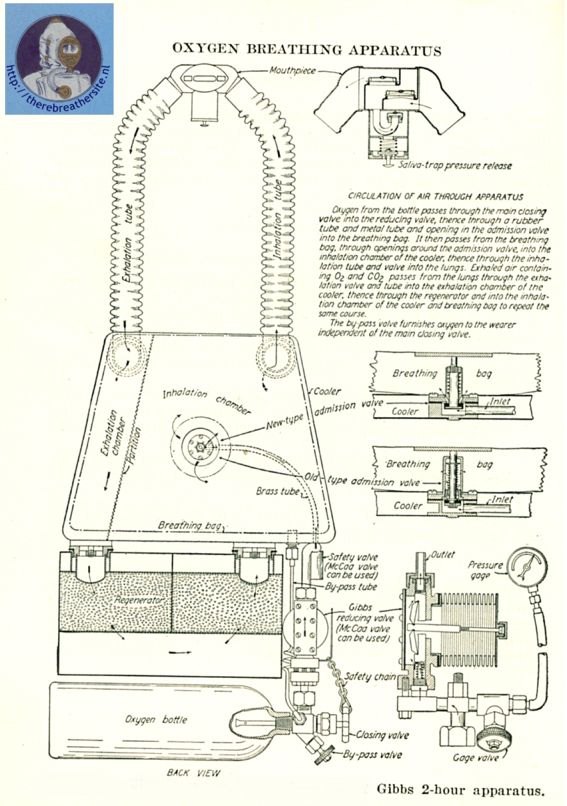
The Gibbs 2-hour apparatus has five main parts:
- A steel cylinder or bottle, with main and bypass valves, containing oxygen under high pressure.
- A reducing valve to reduce high pressure and to supply oxygen from the oxygen bottle to the wearer as required at a pressure slightly higher than ordinary or normal.
- A regenerator containing chemicals for absorbing carbon dioxide.
- A breathing bag and cooler which, with the regenerator, serve as an air reservoir. The breathing bag also operates an auxiliary oxygen-admission valve that is attached to the cooler.
- A mouthpiece, with inhalation, exhalation, saliva-trap, and pressure-release valves and tubes that connect to the cooler.
Oxygen bottle
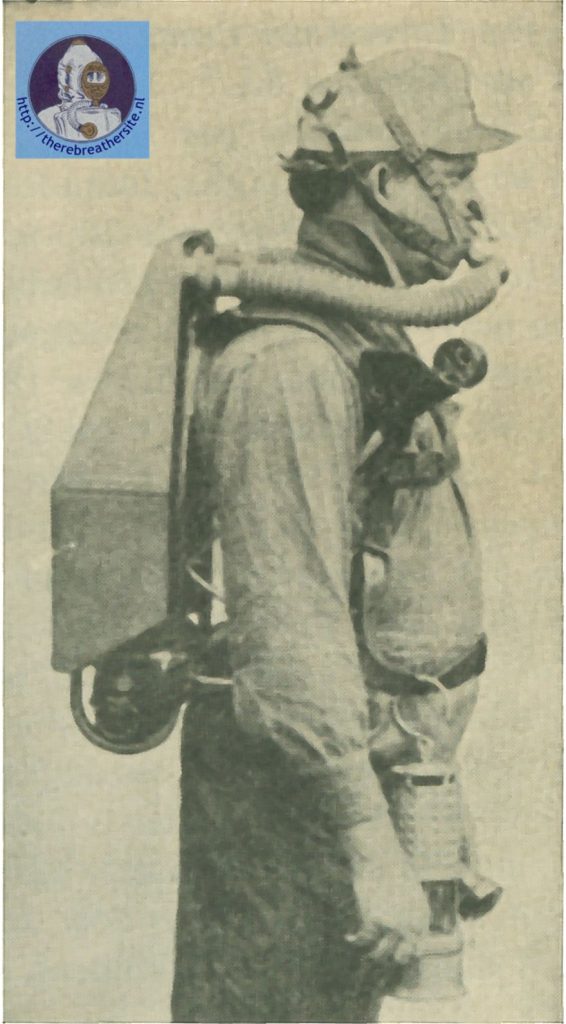
The oxygen bottle is constructed of high-grade carbon steel and tested in accordance with Interstate Commerce Commission Specifications. The bottle, when empty, has a capacity of about 1.8 to 1.0 liters (110 to 116 cubic inches) or about 2 quarts and about 245 liters (8.6 cubic feet) of oxygen when fully charged to 135 atmospheres (1,984.5 pounds per square inch). When fully charged the bottle, including main and bypass valves, weighs about 9 pounds and contains enough oxygen to supply the wearer for at least 2 hours during strenuous exertion. The bottle is attached to the apparatus by threaded connections on the bottom of the reducing valve and the lower end of the bypass tube, which are connected to the outlets of the valves, and by an adjustable metal strap. The main valve should be opened two to four complete turns when the apparatus is being worn (a lock nut and shoulder prevent it from being opened more than four turns), and it should be locked in the open position by a chain and snap hook provided for this purpose. The bypass valve should be opened only in an emergency and then but for a short time. A metal tube with a small opening near its end is attached to the body of the valve and extends several inches into the oxygen bottle, allowing oxygen to flow from the center of the bottle through the main or bypass valves without danger of rust, scale, sediment, or moisture being drawn into the circulatory system. A safety cap filled with Rose’s metal (an alloy of 50 parts bismuth, 28 parts lead, and 22 parts tin, by weight, melting at 94° C.) and containing a frangible copper disk is also attached to the valve body by a threaded connection. This cap provides for escape of oxygen without rupture of the bottle if exposed to fire. The figure shows how the oxygen bottle is attached to the apparatus.
Reducing Valve
The essential parts of the Gibbs reducing valve are a toggle joint equipped with a threaded metal rod, a casenite seat, a metal spring, and a steel nozzle. These parts are placed in a valve housing to which is attached (by a threaded connection) a coiled, cylindrical brass diaphragm or bellows and a high-pressure fitting (by means of three metal bolts). The nozzle extends from the high-pressure fitting into the bottom of the valve housing; the metal spring is placed over the end of the nozzle; the casenite seat is inserted over the spring and the outlet of the nozzle and under the lower part of the toggle joint; and the toggle joint, whose upper part rests against a threaded insert in the upper part of the housing, is connected to the end of the bellows by the metal rod. The reducing valve is attached to the apparatus frame by a threaded projection and a nut on the high-pressure fitting; to the oxygen bottle by a strong threaded connection having a fiber gasket and a copper screen ; and to the oxygen supply and gage tubes by threaded connections. If the reducing valve is properly connected to a charged oxygen bottle, when the main valve is opened oxygen under pressure enters the high-pressure fitting, passes through the nozzle, enters the housing, extends or lengthens the bellows, and operates the toggle joint. If the admission valve is closed when the oxygen is turned on the bellows will be extended to the point where the toggle joint will force the seat tightly on the end of the nozzle, thereby shutting off the flow of oxygen and the pressure from the bottle. As soon as the admission valve is opened to supply oxygen to the wearer the pressure in the bellows is reduced to a small extent and it contracts slightly, removing the seat from the nozzle, and oxygen flows through the reducing and admission valves. Oxygen continues to flow until the admission valve is again closed, pressure is increased, and the reducing valve closes. This cycle is repeated as long as the apparatus is worn or until the oxygen in the bottle is exhausted. Thus, oxygen is supplied automatically as
the wearer requires it; he receives much or little, depending on whether he is working or resting. The reducing valve should lie set to close or “shut off” at a pressure of about 3 pounds per square inch. Two lock nuts, one locking the adjusting screw on the outlet end of the reducing valve and another locking the rod connecting the toggle joint and the bellows, are used to safeguard the valve. No attempt should be made to adjust the adjusting screw, the toggle joint and bellows rod, or the three bolts that connect the high-pressure fitting to the valve housing. If the reducing valve is not operating properly the safest procedure is to return it to the manufacturer for adjustment or repairs. Tampering with these adjustments or making improper adjustment will interfere with operation of the valve and may result in shutting off the oxygen flow completely or destroying the valve. Figure 1 shows details of construction of the Gibbs reducing valve and how it is attached to the apparatus. The McCaa reducing valve, although constructed somewhat differently, is basically the same as the Gibbs reducing valve. It therefore can also be used on the Gibbs apparatus.
Regenerator/Scrubber
The regenerator is a rectangular sheet-copper container or canister. It has two compartments, top and bottom screens, and threaded inserts with screens on the top near each end. These inserts are removed when the regenerator is filled or emptied. When ready for use the regenerator is charged or filled with 4 pounds (2 pounds in each compartment) of cardoxide, which absorbs the carbon dioxide exhaled by the wearer. Cardoxide is a specially prepared chemical; is a highly efficient absorber of carbon dioxide; differs considerably from caustic soda and caustic potash, which were used before it was discovered; and has several outstanding advantages as regenerating material. (See p. 12.) After being filled, the regenerator is fastened to the apparatus by metal screws attached to the cooler, which are screwed into threaded holes la the center of the regenerator inserts. It should l)e removed from the apparatus, emptied, and refilled with fresh cardoxide after each 2-hour wearing period. A charge of cardoxide should not he used longer than one wearing period, particularly in actual recovery work, as cardoxide will not absorb carbon dioxide efficiently over a prolonged period of use. Moreover, when the limit of absorption is reached it “breaks” quickly, and if it is used too long the wearer will develop a severe headache, will he physically affected, and may be overcome. Figure 1 shows details of construction of the regenerator, how it is attached to the apparatus, and how air circulates through the cardoxide in the regenerator.

Breathing Bag
The breathing hag, which is carried on the back, serves as an air reservoir from and into which the wearer breathes. It has one compartment with a capacity of about 8 liters (488 cubic inches) or about 8 quarts when fully inflated. The latest type Gibbs breathing bag is made of high-grade sheet rubber about 3/64 inch thick covered with stockinet, constructed with vulcanized seams so that the bag is virtually one piece of rubber. The top of the bag is attached to the top of the cooler by two screws and by a metal ring having threaded projections in the center of the inside layer of the fabric. This metal ring, when placed over an opening in the center of the cooler, permits free interchange of air between the bag and cooler. The cooler is constructed of sheet metal and cools the purified exhaled air coming from the regenerator. It is divided by a metal partition into two compartments known as the exhalation (small) side and the inhalation (large) side. Attached to the center of the cooler on the exhalation side is the admission valve, which extends through the breathing bag-cooler opening into the bag. This valve is one of the most important features of the Gibbs apparatus and forms part of the opening and closing system of the reducing valve. Connected to the admission valve inside
the cooler is a metal oxygen-supply tube that leads to the bottom of the inhalation side of the cooler and connects with a rubber oxygen-supply tube attached to the reducing valve. When the wearer inhales and the breathing bag is drawn nearly flat, a metal “bumper” plate within the bag strikes the stem or pin of the admission valve and opens it; if the main bottle valve is open oxygen is thereby permitted to flow through the reducing valve, the oxygen-supply tubes, and the admission valve into the breathing bag. From there the oxygen can be drawn into the wearer’s lungs or joins the purified air from the regenerator. When the wearer exhales the breathing bag is inflated or expanded, raising the bumper plate, and the admission valve closes, which closes the reducing valve in turn. A safety valve is attached to the cooler at the point where the oxygen-supply tubes join. This valve is designed to operate at about 7 pounds pressure and at the same time give a whistle warning. Its function is to protect the wearer if the reducing valve fails to shut off at the proper pressure. If the whistle sounds while the apparatus is being worn the wearer should close the main bottle valve, obtain oxygen by means of the bypass valve, and return to fresh air at once. Threaded connections are provided for attaching the upper end of the bypass tube to the inhalation side of the cooler and to connect the inhalation- and exhalation-tube couplings to openings in the top of the cooler. Figure 1 shows details of construction of the breathing bag, cooler, admission and safety valves, and oxygen-supply tubes and how they are attached to each other and to the apparatus.

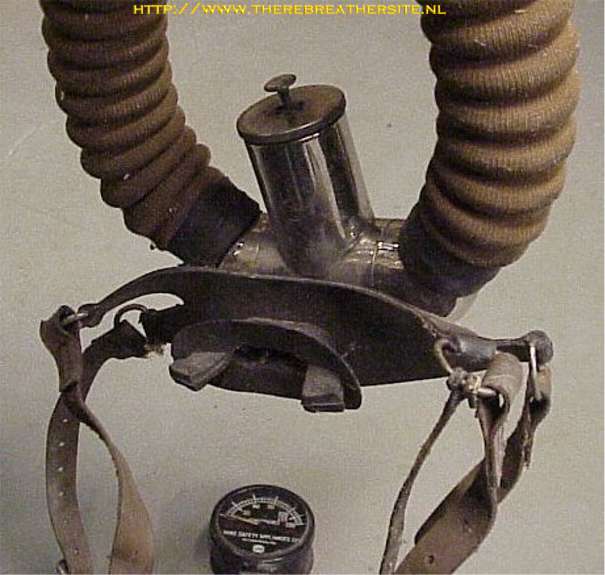
Mouthpiece
The wearer of a Gibbs apparatus breathes entirely through his mouth, as a steel-wire clip closes the nostrils completely. The complete mouthpiece assembly comprises a rubber mouthpiece firmly attached to a T-shape metal mouthpiece housing that contains a horizontal mica-disk inhalation valve; a similar exhalation valve; a U-tube saliva-trap with a mica-disk
valve on the outlet of the tube; and a hand-operated release valve attached by a threaded connection on the bottom outlet of the saliva-trap barrel. Attached to the metal mouthpiece are flexible, corrugated-rubber tubes that connect to the cooler by threaded couplings. When the apparatus is worn, the rubber mouthpiece fits snugly between the lips and teeth of the wearer and is held in place by straps attached to the mouthpiece, which are fastened or buckled to a suitable cap or head strap. When the wearer inhales, the inhalation valve opens and the exhalation valve closes and when he exhales the exhalation valve opens and the inhalation valve closes, compelling the air to circulate through the mouthpiece, breathing tubes, regenerator, cooler, and breathing bag in one direction. The saliva-trap and release valves are so arranged that the wearer can release excess pressure, clear the apparatus of nitrogen, and discharge accumulated saliva to the outside without danger of drawing outside air into the apparatus. When the release valve is operated and the wearer exhales to the outside air, the exhalation breathing tube should always be pinched or squeezed to close it off, thereby forcing the exhaled air through the release valve instead of returning it into the apparatus. Figure 1 shows in detail how the mouthpiece is constructed and how it is attached to the apparatus.
Other Parts
A bypass tube, with one end connected to the outlet of the bypass valve of the bottle valve and the other end to the bottom of the inhalation side of the cooler, is used to supply oxygen to the wearer independently of the main bottle, reducing, safety, and admission valves. Should any or all of these valves fail to operate properly the wearer should open the bypass valve momentarily to obtain oxygen. If this occurs during work in a dangerous atmosphere, he should continue operating the valve in this manner and return to fresh air for adjustment or repair of the apparatus.
A pressure. Rage, graduated in atmospheres and carried in a leather pocket on the front of the right shoulder strap, indicates the pressure in the oxygen bottle and permits the wearer to determine the amount of oxygen remaining. The gage is connected to a flexible, canvas-covered, coiled-metal tube attached to the outlet of the gage valve. A needlepoint valve fastened to the high-pressure fitting of the reducing valve controls admission of oxygen into the gage tube and gage.
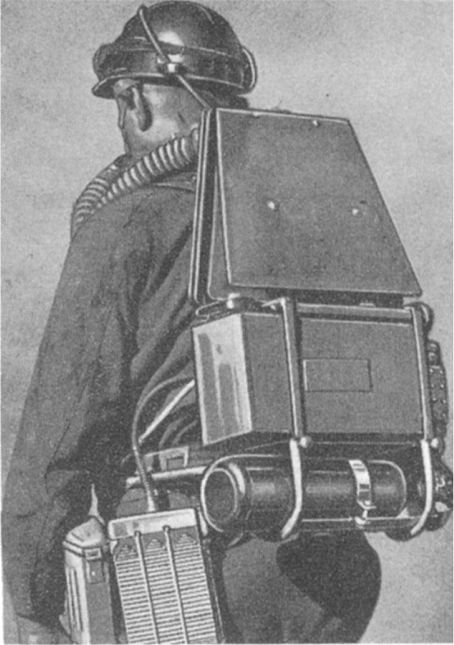
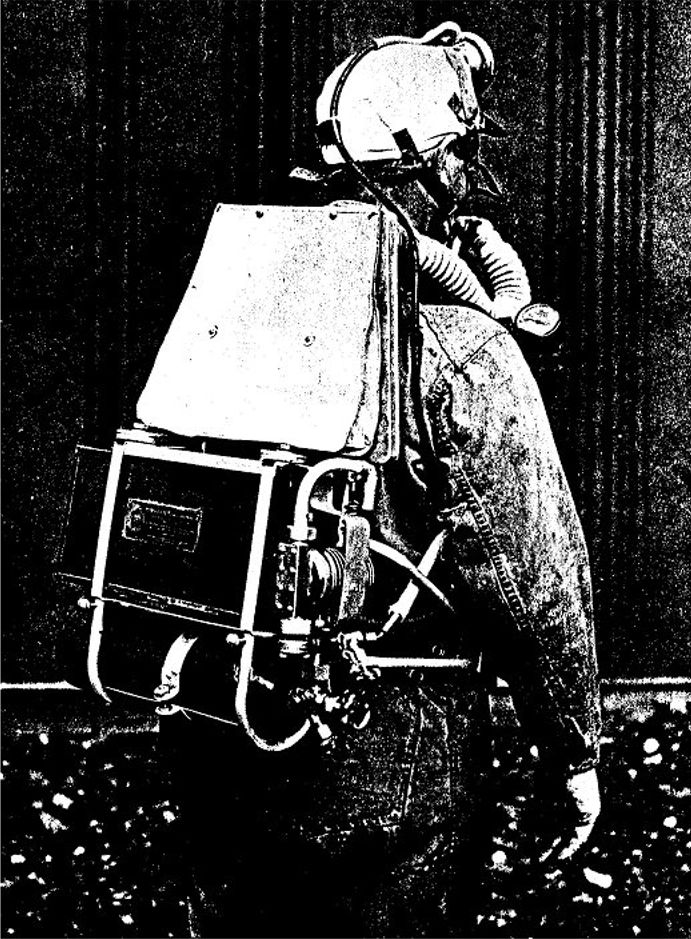
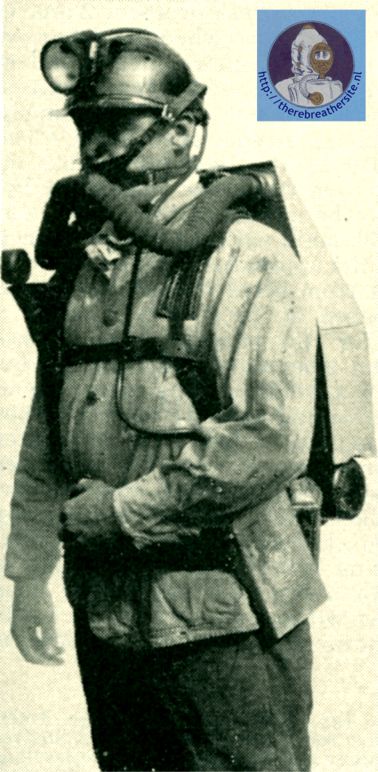
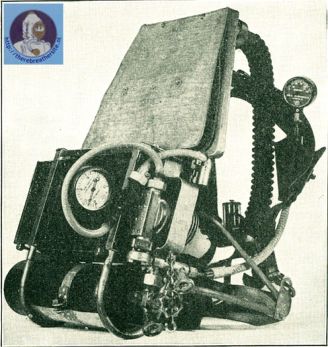
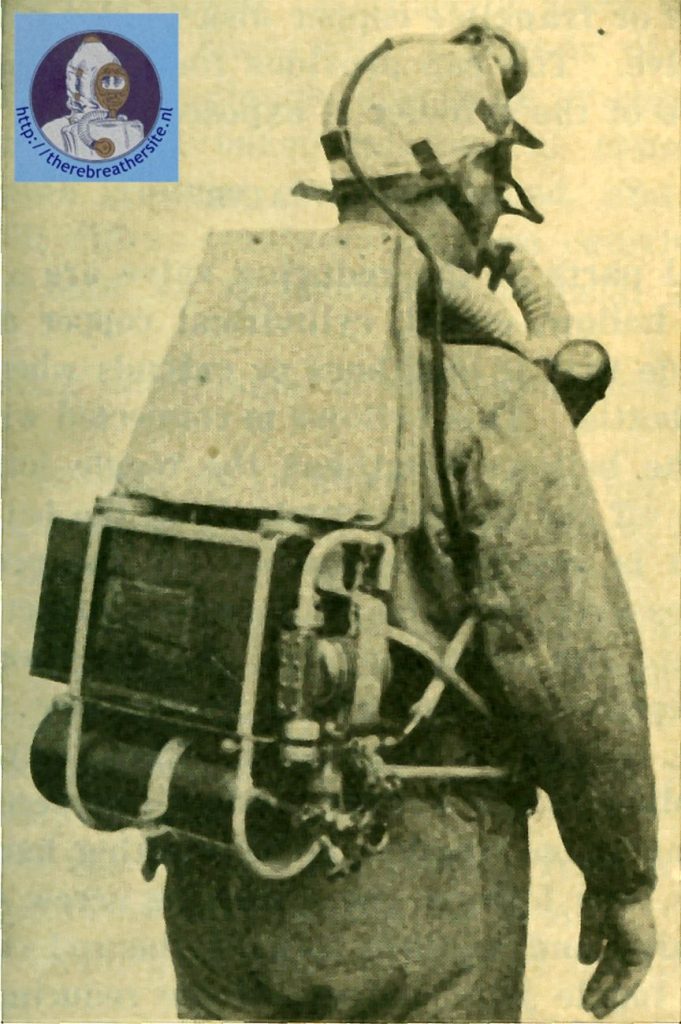
A sheet-metal cover over the breathing bag, cooler, regenerator, reducing valve, and other vital parts protects them against direct blows and falling material. The various parts of the apparatus are attached to a rigid, tubular, metal frame or to other parts connected to the frame. An adjustable padded-leather harness consisting of body and shoulder straps supports the apparatus and attaches it to the wearer. The complete apparatus, fully charged, weighs about 38 pounds.

Circulatory System
Oxygen and air circulate through the Gibbs apparatus as follows: When the main bottle valve is opened, oxygen passes through it into the reducing valve, into the rubber oxygen-supply tube, into the metal oxygen-supply tube enclosed in the cooler, into the admission valve attached to the center of the cooler, and into the breathing bag.1” The oxygen leaves the breathing hag through openings around the admission valve, enters the inhalation side of the cooler, and is drawn by the wearer into the inhalation tube, through the inhalation valve, into the mouthpiece, and into the lungs. Exhaled air containing unused oxygen and carbon dioxide passes into the mouthpiece, through the exhalation valve, into the exhalation tube, into the exhalation side of the cooler, into the regenerator, and into the inhalation side of the cooler to repeat the cycle, fresh oxygen being supplied from the bottle through the reducing and admission valves as required. When the bypass valve is opened, oxygen passes through the bypass tube into the inhalation side of the cooler and the breathing bag and from there i.s drawn into the lungs. When the gage valve is open and the main bottle valve is opened oxygen passes into the coiled-metal gage tube and into the pressure gage, which indicates the pressure in the oxygen bottle. Figure 1 shows details of the circulation of oxygen and air in the apparatus.
Consumption of Oxygen
A Gibbs 2-hour apparatus when fully charged (135 atmospheres) will last the wearer about 15 hours if at complete rest and 2 hours or more if he does the utmost physical work possible in that time. The apparatus actually has furnished a wearer 5 liters of oxygen per minute over a 5-minute period of particularly violent exertion, it being impossible for him to continue the test much longer on account of physical limitations. With the admission valve open and oxygen flow unobstructed a fully charged Gibbs apparatus will feed about 20 liters or quarts (1,220 cubic inches) of oxygen per minute, an amount considerably more than a wearer can consume. The oxygen supply of a fully charged apparatus would therefore be exhausted in about 12 minutes if allowed to flow freely to the outside air. To determine the flow, attach a tube from the inhalation side of the cooler to a flow meter or measuring bag; with the main bottle valve open hold the admission valve open for 1 minute, and measure the amount of oxygen that passes through the admission valve.

Accumulation of Nitrogen
The oxygen sold by manufacturers and dealers for use in oxygen breathing apparatus is usually about 98 to 99 percent oxygen and about 1 to 2 percent nitrogen. This nitrogen, with that in the air in the lungs, is fed into the apparatus with the oxygen and exhaled air; as it is not absorbed by the lungs or chemicals in the apparatus it accumulates in the breathing bag and other parts of the apparatus unless let out by a release valve or other means. Consequently, if an apparatus wearer starts with normal air, containing 20.93 percent oxygen and about 79.00 percent nitrogen or even a relatively .high percentage of oxygen, in his apparatus and if he does not periodically operate a release valve or similar device to dispose of the nitrogen the percentage of oxygen in the air breathed will be lowered gradually by the inflowing nitrogen. Sooner or later the wearer will be overcome, often without warning, and will collapse because of insufficient oxygen. The apparatus should therefore be cleared of residual or normal air and filled with relatively pure oxygen by the wearer before he puts on the nose clip. Moreover, the wearer should use the relief valve by exhaling through it to the outside air about every 15 or 20 minutes while wearing the apparatus to eliminate accumulations of nitrogen and saliva, as there is always a possibility that commercial oxygen may contain over 2 percent nitrogen. If the directions in test 12 (p. 46), containing detailed information on the elimination of nitrogen and saliva from the apparatus, are followed and if the wearer exhales properly, the air breathed by the wearer of a Gibbs apparatus will contain at least 75 percent oxygen and not over 25 percent nitrogen. New apparatus bottles or bottles in which valves have been replaced should be fully charged to 135 atmospheres, discharged to the outside air until almost empty, and refilled. Any residual nitrogen in the bottles can be eliminated thereby.
Resistance to breathing
The resistance to breathing in any apparatus should never exceed 2 inches of water gage while hard work is being performed for a 2-hour period. If resistance is high the exhalation valve may fail to operate properly; the wearer will then breathe part of the air just exhaled and therefore unpurified. An excess of carbon dioxide accumulates in the lungs, hindering absorption of oxygen by the blood and tiring the respiratory system. As the carbon dioxide increases the rate of breathing increases, the depth of breathing decreases, and the wearer becomes nauseated or even collapses. Moreover, an apparatus wearer who has been breathing against undue resistance may be sore in the chest or hack for several days. In the Gibbs apparatus the pressure in the breathing bag; when the wearer is not inhaling or exhaling is approximately one-half inch of water gage and, when exhalation is forced, approximately 1.5 inches. When an apparatus wearer breathes deeply with the admission valve properly adjusted the pressure Is about one-fourth inch of water gage. These pressures are not high enough to affect, the wearer noticeably, even after a number of 2-hour periods of strenuous apparatus work.
Temperature of Inhaled gas
The cooler on the Gibbs apparatus usually keeps the air at a temperature low enough to avoid discomfort or difficulty from heat. However, if the wearer works hard or the mine temperature is high the air supplied by this or other types of apparatus may in time become uncomfortably warm.
Positive Pressure apparatus
The Gibbs apparatus has a slight outward or positive pressure in all parts of its air-circulating system. The danger from negative pressure is that if the apparatus leaks while the wearer is in irrespirable gases these gases will be drawn into the circulated air with serious and possibly fatal results.
Test of apparatus
All oxygen breathing apparatus should be tested frequently between periods of actual use to determine their condition and should be tested carefully as to air tightness and working order before they are worn in irrespirable or poisonous gases. All leaks found during tests should be properly repaired and all defective parts repaired, adjusted, or replaced before the apparatus is used. It is extremely dangerous to wear an apparatus in irrespirable air when it is not working properly or is leaking. The following tests will show if the Gibbs apparatus is ready for use :
1.Test for moisture in oxygen bottle
After the oxygen bottle or cylinder has been charged to about 1,984.5 pounds per square inch (13o atmospheres) hold it in a vertical position with the valves down. Open the main valve, and close it quickly. Water blown from the valve shows that moisture has gathered in the bottle. Remove accumulations of moisture, sediment, rust, or scale by taking the valves out of the bottle and draining and cleaning the bottle. Forcing or carrying water or sediment into the reducing valve or apparatus is dangerous.
2. Test for tightness of oxygen bottle-valves
To test the main bottle valve firmly attach a metal cap provided for this purpose to the outlet of the valve of a charged bottle, and open the valve; then immerse the valve and the neck of the bottle in water. Escaping air bubbles around the valve stem, packing gland, or bottle connection indicate leaks. Then close the main valve, remove the metal cap, fond again immerse the outlet of the valve in water. Air bubbles indicate that the valve is not closed tightly or that it has a defective seat. Repair all leaks and repair, adjust, or replace all defective parts found during either test before the bottle is used. Test the bypass valve in the same manner as the main valve. After determining that there are no leaks In the valves and the bottle connection place the fully charged bottle in the frame of the apparatus (making sure that the reducing-valve gasket and the copper screen in the reducing-valve oxygen-bottle connection are in place, clean, and in good condition), and attach the reducing-valve connection firmly to the outlet of the main bottle valve. Then attach the bypass-tube connection snugly to the outlet of the bypass valve, and tighten the metal strap attached to the apparatus around the center of the oxygen bottle.
3. Test for pressure reducing valve
With the oxygen bottle properly attached to the reducing valve disconnect the oxygen-supply tube from the outlet of the reducing valve, and attach a low-pressure gage (fig. 3) to the reducing-valve outlet. Next, with the outlet valve of the low-pressure gage closed open the main bottle valve, and read the low-pressure gage, which will now show the pressure (shut-off pressure) in the reducing valve. The pressure reading should be about 3 pounds and should not be below 2 or above 5 pounds. If the shut-off pressure of the reducing valve is too high or too low replace the valve.
4. Test for tightness of reducing valve, gage valve, gage tube and gage
With the main bottle valve open and the low-pressure gage still attached open the high-pressure-gage valve (if not already open), and read the high-pressure gage, which will now show the pressure in the oxygen bottle. Then close the main bottle valve. If there are leaks in the reducing valve, gage valve (open position), gage tube, gage, and their connections the hands of both the high- and low-pressure gages move toward zero. Locate leaks by brushing soapsuds over the parts and connections under pressure. Repair all leaks and repair, adjust, or replace all defective parts before the apparatus is used. Always replace a defective reducing valve instead of attempting repairs. After determining that there are no leaks close the high-pressure-gage valve, and allow the oxygen to escape from the reducing valve by opening the low-pressure-gage valve. This traps oxygen under high pressure between the high-pressure-gage valve and the gage. If the high-pressure-gage valve leaks the gage hand moves toward zero; if this happens, repair or replace the valve. After determining that no leaks are present in the high-pressure-gage valve (closed position) open it, and allow the trapped oxygen to escape.
5. Test for pressure of oxygen flow of reducing valve
With the low-pressure gage still fastened to the reducing valve attach the outlet of the gage to the oxygen supply tube, and open the low-pressure-gage valve. Then open the main bottle valve, and open the admission valve by pressing against the metal plate of the breathing bag. This allows oxygen to flow through the reducing and admission valves, and the low-pressure gage will indicate the flow pressure. The oxygen-flow pressure for a reducing valve in good condition should be % to 1 pound. Read the low-pressure gage, and determine the flow pressure; then close the admission valve by raising the metal plate away from the admission valve. If the oxygen-flow pressure is not satisfactory replace the reducing valve.
6. Test for operation and tightness of safety valve
With the low-pressure gage still attached to the reducing valve and oxygen-supply tube, the low-pressure-gage valve open, the admission valve closed, and the main bottle valve open press or squeeze the reducing-valve bellows inward until the reducing-valve seat opens. This allows oxygen to flow into the reducing valve, the low-pressure gage, and the safety valve until a pressure is reached that will cause the safety valve to whistle or blow off, relieving the increased pressure. The safety valve should leak at about 6 pounds and whistle or blow off at about 7 pounds pressure. Observe the low-pressure gage,
and note—as the pressure builds up—the pressure at which the safety valve operates. Determine that the safety valve is operating properly; then open and quickly close the admission valve to let the excess pressure escape. Again observe the low-pressure gage; if the safety valve leaks the hand of the gage moves toward zero. Locate leaks by brushing soapsuds over the valve or by immersing it in a glass of water. Repair all leaks and repair, adjust, or replace all defective parts before the apparatus is worn. Determine that the safety valve is operating properly and that no leaks are present; then close the main bottle valve and open the admission valve to let trapped oxygen escape. Remove the low-pressure gage, and connect the oxygen-supply tube (making sure the gasket is in place and in good condition) to the outlet of the reducing valve.
7. Test for tightness of admission valve
Close the admission valve by raising the metal plate of the breathing bag (low-pressure gage not attached), and open the main bottle valve. Then, with the high-pressure-gage valve open read the high-pressure gage, and close the main bottle valve. If leaks are present the gage hand moves toward zero. If the gage hand travels toward zero quickly open and close the admission valve several times to blow out dirt that may be lodged tinder the valve seat; if the” leaks continue cover with soapsuds all parts and connections under pressure, from the admission valve to the oxygen bottle, including the gage tube and gage. If the leaks cannot be located by doing this the admission valve is doubtless leaking; determine this definitely by removing the breathing bag and brushing soapsuds over the admission valve while it is under pressure.
Stop all leaks by cleaning, repairing, or replacing the admission valve before the apparatus is worn. If the gage hand remains stationary after the main valve is closed, this test also shows that the safety valve, oxygen-supply tubes, reducing valve, gage valve, gage tube, gage, and all other parts and connections between the oxygen bottle and admission valve are tight. Always make this test just before the apparatus is worn, as it shows quickly if the parts of the apparatus under high and intermediate pressure are tight.
8. Test for tightness of cooler partition
Seal the bottom inhalation and exhalation openings of the cooler with solid connections, and close the top opening of the inhalation side with the palm of the hand ; or connect a water gage to the opening, and blow into the top opening on the exhalation side. If no pressure can be noticed at the top opening of the inhalation side, the partition is tight. Another method is to block the bottom opening on the exhalation side and blow in the top opening. However, it may be difficult, if not impossible, to ascertain by this method if small leaks are present. If the cooler partition leaks repair or replace the cooler before the apparatus is worn.
9. Tests for tightness of cooler, Regenerator, Breathing bag, and bypass tube, and of circulation and resistance
Connect the regenerator firmly to the inhalation and exhalation sides of the cooler, making sure that the gaskets are in place and in good condition, and block the top opening of the inhalation side of the cooler with the palm of the hand or a solid plug. Next, exhale forcibly several times in the top opening of the exhalation side to inflate the breathing bag. Then press slightly on the inflated breathing bag: if leaks are present in the cooler, regenerator, breathing bag, and bypass tube and their connections the breathing bag will deflate or collapse. Locate leaks by brushing soapsuds over the parts under pressure or by immersing them in water. (Also test cooler, regenerator, and breathing bag when detached from the apparatus by closing openings and immersing them in water while under pressure.) Repair all leaks and repair, adjust, or replace all defective parts before the apparatus is used. Determine that no leaks are present; then blow into the top opening on the exhalation side of the cooler, with the regenerator in place, and note if air issues freely from the top opening of the inhalation side. If there is no appreciable resistance to breathing through the cooler, regenerator, and breathing bag it shows that air circulation is proper and complete. Forced breathing indicates undue resistance and probably a defective or blocked regenerator, which should be corrected by careful repairs or replacement before the apparatus is worn.
10. Test for tightness and operation of mouthpiece, valves and tubes
With the inhalation and exhalation tubes and their connections and the rubber mouthpiece attached securely to the metal mouthpiece, place a solid plug in the opening of the exhalation coupling and the thumb firmly over the rubber mouthpiece opening, and immerse all of the parts, except the inhalation-tube coupling, in water. Then exhale forcibly in the opening of the inhalation-tube coupling. Air bubbles indicate leaks. Next, with the solid plug still in the exhalation coupling (or the opening blocked), place the end of the inhalation tube under water, and exhale forcibly into the mouthpiece. Air bubbles coming from the end of the inhalation tube indicate that the inhalation valve leaks. Then remove the solid plug from the exhalation-tube coupling, place the mouthpiece under water, and exhale forcibly in the opening of the exhalation tube. Air bubbles coming from the mouthpiece indicate that the exhalation valve leaks. Next, place the rubber mouthpiece in the mouth, and inhale and exhale through it quickly several times to see that the mica-disk inhalation and exhalation valves are working properly, that they open and close freely, and that they have a clear, ringing sound. Remove the bottom of the saliva trap containing the release valve from the metal mouthpiece, immerse the rubber mouthpiece in water, and exhale forcibly in the saliva-trap barrel. Air bubbles issuing from the mouthpiece indicate that the mica-disk valve in the saliva trap is leaking. Next, replace the release valve on the saliva trap, milking sure the gasket and spring are in place and in good condition, and operate the plunger of the valve several times to make sure it works freely. Replace the solid plug in the exhalation-tube coupling, immerse the release valve in a glass of water, and exhale forcibly into the rubber mouthpiece. Air bubbles issuing from the release valve indicate leaks. Remove the solid plug from the exhalation-tube coupling, and carefully examine the rubber mouthpiece, breathing tubes, and the nose clip. Bend the mouthpiece and tubes in various directions to make sure that they are flexible and that there are no defects, and bend the nose clip to see that it has enough spring. Finally, place the nose clip on the nose, and attempt to inhale and exhale deeply through the nose. If the clip is adjusted properly breathing through the nose will be impossible. Repair all leaks and repair, adjust, or replace all defective parts found during the tests before the mouthpiece and tubes are used. Determine that there arc no leaks in the mouthpiece and tubes and that the valves art operating properly; attach them firmly to the cooler (making sure the gaskets are in place and in good condition) by means of the breathing tube-cooler connections.
11. Tests for tightness of assembled apparatus
Check the completely assembled apparatus for air tightness; after the previously described detailed tests of the various parts have been made by the two following tests:
- High- (and intermediate-) pressure side.—Close the admission valve by raising the breathing bag, and open the main bottle valve; then, with the gage valve open, read the high-pressure gage, and close the main bottle valve. Keep observing the gage; if the hand remains stationary after the main bottle valve has been closed the parts (high- and intermediate-pressure side) under pressure— admission valve, safety valve, reducing valve, gage valve, oxygen-supply and gage tubes, gage, and all connections from the admission valve to the oxygen bottle—are tight.
- Low-pressure side.—Exhale repeatedly into the mouthpiece to inflate the breathing bag, then slip the mouthpiece out of the mouth, and quickly block the mouthpiece opening with the thumb; or inflate the breathing bag by opening the main bottle valve, blocking the mouthpiece opening, and pressing on the admission valve or by momentarily opening the bypass valve. Then press on the breathing bag to develop pressure within the parts under test. If the breathing bag remains fully inflated it shows that the parts (low-pressure side) under pressure—mouthpiece, breathing tubes, cooler, regenerator, breathing bag, bypass tube and their connections—are tight.
Always make these two tests just before the apparatus is worn; if no leaks are found it shows that the completely assembled apparatus is tight and free of leaks. Locate leaks by brushing soapsuds over the parts under pressure. Repair all leaks and repair, adjust, or replace all defective parts before the apparatus is worn in irrespirable air.
12. Removal of excess nitrogen and tests for operation of apparatus
After the completely assembled apparatus has been tested and found to be fully charged, airtight, and in good condition attach the cover to the apparatus, put on the apparatus, and adjust the body straps to fit. Then place the rubber mouthpiece in the mouth, adjust it, and fasten it snugly in place with the mouthpiece straps and the buckles of the hat, cap, or special strap. Inhale deeply from the apparatus, and exhale through the nose to the outside air at least four times to empty the apparatus completely of normal air. Then open the main bottle valve, inhale from the apparatus and exhale through the nose to the outside air at least three times (o inflate the breathing bag by momentarily opening the bypass valve, and inhale from the apparatus and exhale to the outside at least three times), and place the nose clip snugly on the nose. Then open the bypass valve momentarily to make sure it is working properly. Finally, firmly pinch the exhalation tube to provide resistance; open the release valve on the mouthpiece; and exhale forcibly to the outside air throng the open valve to make sure it is working properly. Repeat this procedure (pinching the exhalation tube, opening the release valve, and exhaling to the outside air) three or four times every 15 or 20 minutes to dispose of accumulated nitrogen and saliva. Completely emptying the apparatus of normal air before turning on the oxygen, inhaling from the apparatus and exhaling to the outside before the nose clip is put on, and exhaling to the outside periodically while the apparatus is being worn are extremely important. If the directions a followed properly nitrogen and saliva will not accumulate, and the wearer will be provided with air containing a high percentage of oxygen.
After the apparatus has been adjusted to the wearer andcleared of nitrogen it may be worn for about 5 minutes in a room filled with formaldehyde or dense smoke. If no fumes are detected in the inhaled air, the breathing is easy, and the apparatus is operating properly it can be trusted to give satisfactory service during a wearing period in poisonous or irrespirable gases. If a smokeroom is not available during recovery operations (which is generally the case), or even if the apparatus has been worn in a smokeroom, the following test should be made to duplicate or supplement the smokeroom test: After opening the main closing valve, clearing the apparatus of nitrogen, adjusting the nose clip, and reading the pressure gage of their apparatus, members of the crew should travel a short distance ahead of fresh air and stop for about 5 minutes to see that the apparatus are ‘airtight and working properly before exploring or working in irrespirable or poisonous gases. If leaks are detected in any apparatus the entire crew should return to fresh air immediately. Before the apparatus are worn in irrespirable air the main bottle valve should always be locked open by attaching the safety chain.
Time required for tests
A man properly trained in the use of the Gibbs apparatus should be able to make the 10 tests of the various parts of the apparatus as described and examine rubber parts for wear and deterioration in about 15 or 20 minutes, using approximately 10 atmospheres of oxygen. When the apparatus is kept fully charged, maintained in good condition, and tested regularly and frequently a man well-trained in its use can determine within 1 minute, by making the two tests of the completely assembled apparatus, whether it is safe for use in irrespirable or poisonous gases.

Therebreathersite was founded by Jan Willem Bech in 1999. After a diving career of many years, he decided to start technical diving in 1999. He immediately noticed that at that time there was almost no website that contained the history of closed breathing systems. The start for the website led to a huge collection that offered about 1,300 pages of information until 2019. In 2019, a fresh start was made with the website now freely available online for everyone. Therebreathersite is a source of information for divers, researchers, technicians and students. I hope you enjoy browsing the content!